Prevalence of Temporomandibular Joint Disorders Among Dental Patients in a Private Institution
Abstract
Temporomandibular joints (TMJ) are the bilateral synovial articulation between temporal bone and lower jaw, seen on each side of the jaws. Temporomandibular joint disorders (TMD) can be defined as the tenderness of the jaws and dysfunction of the associated muscles of mastication and the temporomandibular joints, which connect the mandible to the skull. The exact cause of TMD still remains mysterious and unclear. However, the possible attributes of TMD are arthritis, trauma or blow to the TMJ, excessive gum chewing and bruxism. Patients are usually treated with ice packs, gentle massage at the jaw area and prescription of nonsteroidal anti-inflammatory drugs (NSAIDs). This study sought to evaluate the incidence rate, age and gender differences of TMD among patients reporting to Saveetha Dental College and Hospital. The following parameters were evaluated based on the dental records; age, gender and types of TMD. Excel tabulation and SPSS version 23 was used for data analysis. The prevalence of temporomandibular disorders was higher in female patients (51.9%) than male patients (48.1%). The most frequent age group affected by temporomandibular disorders was 31-40 years (36.7%). Disc-condyle disorder (75.9%) is the most frequent sub-type of temporomandibular disorders present in the patients. There was no statistically significant correlation between age and TMD (p=0.847); and gender and TMD (p=0.365). It can be concluded that within the limits of study, TMD was present in adulthood and was more common in women, with disc-condyle disorder being the most prevalent type.
Keywords
Myofascial Pain, Prevalence, Temporomandibular Disorders, Temporomandibular Joint
Introduction
According to the American Academy of Temporomandibular Disorders, “temporomandibular disorders or dysfunctions (TMD) is a collective term that encompasses many clinical problems involving the masticatory muscles, the temporomandibular joints (TMJ) and associated structures or both” (American Academy of Orofacial Pain, 1993; Silveira, Feltrin, Zanetti, & Mautoni, 2007). It collectively involved the pain and fatigue of cranio-cervico-facial muscles with the irregular of mandibular movement and clicking sound (Habib et al., 2015). The incidence rate of TMD and associated structures are oftentimes seen in childhood and adolescence than that in adulthood. Also, the American Academy of Pediatric Dentistry recognizes that TMJ disorders in childhood presents with mild signs and symptoms (Sönmez, Sari, Oray, & Çamdeviren, 2001).
In general, TMD can be classified into articular and nonarticular disorders, also known as intracapsular and extracapsular, respectively. Myopathies, myofascial pain, fibromyalgia and muscle strains are the scope of nonarticular disorders. The most common nonarticular disorder is presented as myofascial pain that is mainly caused by the extreme activity of clenching and parafunctional habits. Articular disorder is related to the disc-condyle relationship, which is further divided into inflammatory and non-inflammatory arthropathies. They are osteoarthritis, trauma, ankylosed disc, rheumatoid arthritis and pseudogout. The interference between mandibular condyle and articular disc may produce popping sound during jaw opening or closing (Rossi, Greenberg, Liu, & Steinkeler, 2014).
The reported prevalence of TMD in adolescence and adulthood is within the range of 4.9% to 60% with the incidence increasing with age. Studies demonstrated most adults reported features of TMD developed since childhood (Bertoli et al., 2018). The symptoms of TMD include tenderness in the areas of head and face, preauricular and cervical spine, muscle fatigue of craniofacial and mastication region and irregularity of jaw movement and articular sounds (CRANIO®, 2003; Callahan, 2000; Dimitroulis, 1998; Minghelli et al., 2014). Studies showed that painful symptoms in TMD are reflected by the spasm of the muscles of mastication, which is mainly due to postural deviation, malocclusion, parafunctional habits such as clenching of teeth, masticatory muscular dysfunction and emotional disturbances (Dimitroulis, 1998; Roda, Bagan, Fernández, Bazán, & Soriano, 2007). Psychological factors such as anxiety, stress and depression also account for the pathogenesis of TMD. The painful symptom of TMD becomes more severe in people that are highly related with aggravation of emotional tension (Minghelli et al., 2014). The functional balance between teeth occlusion, muscles of mastication and TMJ are disturbed and deranged, attributing to the combination of postural, structural and psychosocial factors (Silva, Lameira, Bérzin, & Silva, 1993).
The pathogenesis of TMD related to emotional distress can be explained when severe forms of tension can develop constant teeth clenching, thereby alteration of ions in cell membranes and local muscle circulations. This mechanism results in pooling of lactic and pyruvic acids, in turn, leads to the stimulation of pain receptors (Cestari & Camparis, 2002). The complex etiologies, wide variation of clinical features and its requirement of multiple diagnostic methods and therapeutic management to reduce the symptoms are the importance that has led to the increase of studies based on the epidemiology and etiopathogenesis of TMDs (Boever & Steenks, 1996). In regards to the above matter, more and more epidemiological studies of TMDs have been conducted over the decades with the association of patient and nonpatient population. Schiffman et al. showed that more than 60% of the subjects have one TMD sign and an estimated 35% mild TMD symptoms (Fricton, Kroening, & Hathaway, 1988).
Our previous publications had been covered on clinical trials (Abhinav, Selvarasu, Maheswari, & Taltia, 2019; Abhinav, Sweta, & Ramesh, 2019; Christabel et al., 2016; Jesudasan, Wahab, & Sekhar, 2015), prospective studies (Jain et al., 2019; Kumar, 2017; Marimuthu et al., 2018; Patil, Durairaj, Kumar, Karthikeyan, & Pradeep, 2017; Rao & Kumar, 2018), systematic reviews (Kumar, 2017; Packiri, 2017) and epidemiological surveys (Kumar & Sneha, 2016; Patturaja & Pradeep, 2016; Rahman & Kumar, 2017; Rahman, 2017). Considering the lack of retrospective studies investigating the prevalence of TMDs based on the types of similar population, thus this study was aimed to evaluate the incidence rate, age and gender differences of TMDs among patients reported to the Saveetha Dental College and Hospital.
MATERIALS AND METHODS
Study design and Study setting
This retrospective cross-sectional study was conducted in Saveetha dental college and hospital, Saveetha University, Chennai, to evaluate the prevalence of temporomandibular joint disorders among dental patients reporting from June 2019 to March 2020. The study was initiated after approval from the institutional review board and it was covered by the following ethical approval number; SDC/SIHEC/2020/DIASDATA/0619-0320.
Study population and sampling
Inclusion criteria for the study were patients with no history of orthodontic treatment and at least 11 years old. Exclusion criteria included history of trauma to the TMJ, immunocompromised patients, having dental prostheses, dental anomalies, systemic diseases with cognitive problems and speech problems, missing or incomplete data. After assessment in the university patient data registry, case records of 79 patients who were diagnosed with TMD and were eligible for the study were included in the study. Cross verification of data for errors was done with the help of an external examiner.
Data collection
Data regarding patients having TMD were retrieved after analyzing 86000 case sheets. The following parameters were evaluated based on the dental records; age, gender and types of TMD. Chief complaints, medical and dental history and treatment report of the patients were examined for the data collection. Patients diagnosed with TMD were further classified into disc-condyle disorder, degenerative disorder and myofascial pain and dysfunction syndrome (MPDS).
Statistical Analysis
The collected data was validated, tabulated and analysed with Statistical Package for Social Sciences for Windows, version 23.0 (SPSS Inc., Chicago, IL, USA) and results were obtained. Categorical variables were expressed in frequency and percentage; and continuous variables in mean and standard deviation. Chi-square test was used to test associations between categorical variables (age, gender and types of TMD). P-value < 0.05 was considered statistically significant.
RESULTS AND DISCUSSION
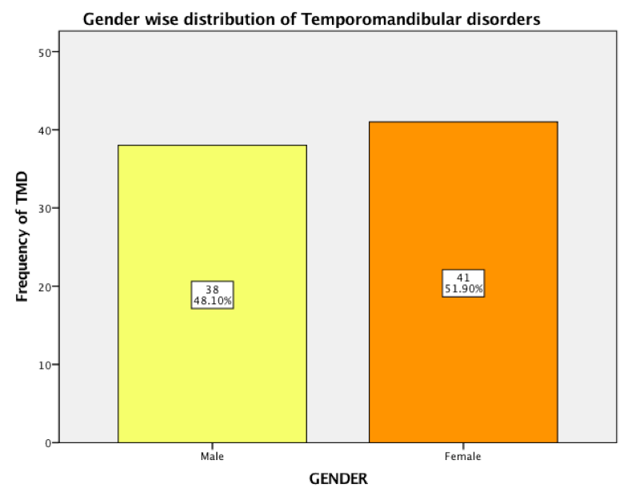
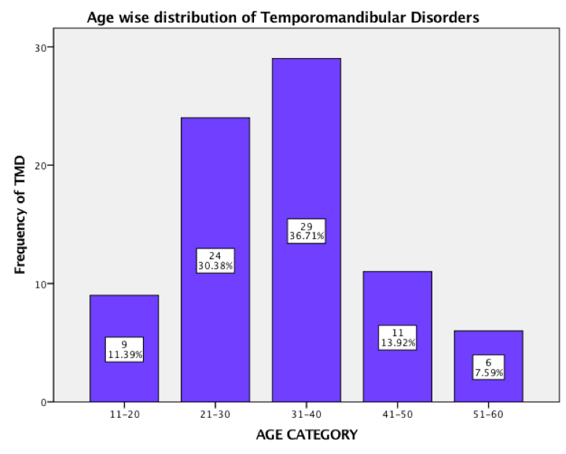
In this study, we evaluated the incidence of TMD among the patients attending our college and its association with gender and age groups. The prevalence of temporomandibular disorders was higher in female patients (51.9%) than male patients (48.1%). X-axis represents the gender male or female while, Y-axis represents the number of patients with TMD. Yellow denotes males and oranges denotes females. TMD was present slightly more in Females (51.9%) compared to males (48.1%) [Figure 1]. The most frequent age group affected by temporomandibular disorders was 31-40 years (36.7%). X-axis represents age groups. Y-axis represents the number of patients with TMD. TMD was observed more in the age group of 31-40 years (36.71%), followed by 21-30 years (30.38%), 41-50 years (13.92%), 11-20 years (11.39%) and 51-60 years (7.59%) [Figure 2].
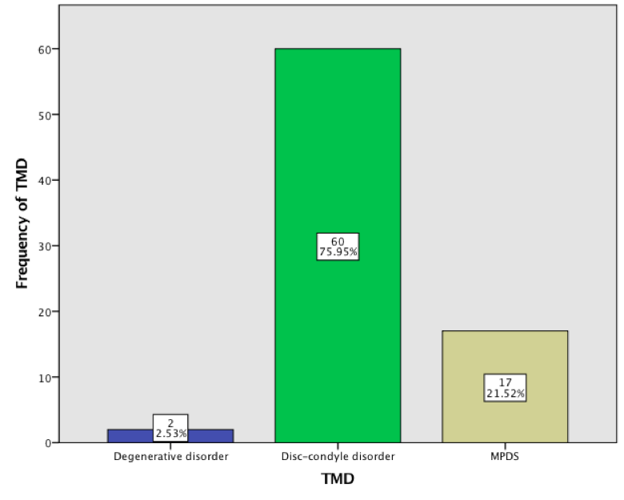
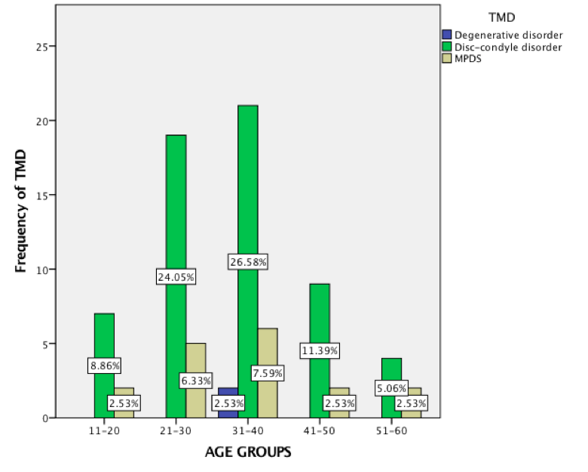
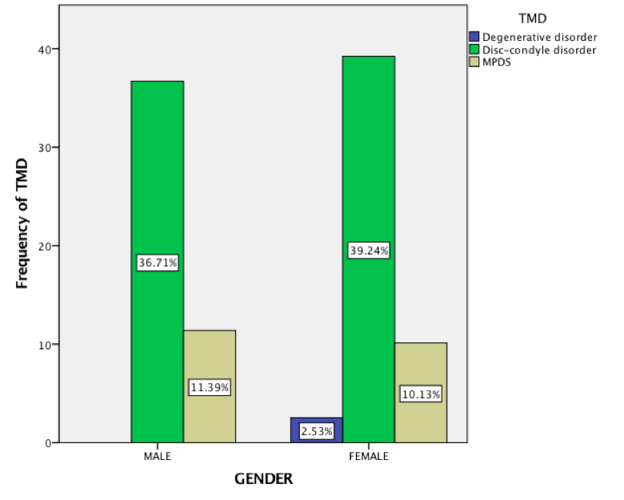
Disc-condyle disorder (75.9%) is the most frequent sub-type of diagnosed temporomandibular disorders and the least recorded was degenerative disorders that were seen only in two patients. X-axis represents the types of TMD. Y-axis represents the number of patients with TMD. Beige denotes MPDS, green denotes disc-condyle disorder and blue denotes degenerative disorder. Disc-condyle disorders (75.95%) was predominantly present among the patients followed by MPDS (21.52%) and degenerative disorder (2.53%) [Figure 3]. There was increased prevalence of degenerative and disc-condyle disorders in females than in male subjects. However, there was no statistical significant correlation of TMDs in different ages and gender. X-axis represents age groups and Y-axis represents frequency of patients with different types of TMD. Beige denotes MPDS, green denotes disc-condyle disorder and blue denotes degenerative disorder. Chi-square test was done and association was found to be statistically not significant between age groups and TMD. Chi-square test value - 4.113, p=0.847 (>0.05). Disc-condyle disorder was predominantly present among all age groups compared to other types of TMD, however this was statistically not significant. X-axis represents gender and Y-axis represents frequency patients with TMD. Beige denotes MPDS, green denotes disc-condyle disorder and blue denotes degenerative disorder. Chi-square test was done and association was found to be statistically not significant between gender and TMD. Chi-square test value - 2.014, p=0.365 (>0.05) and the results are statistically not significant. Females (39.24%) presented with a slightly higher number of disc-condyle disorders compared to males (36.71%), however this was statistically not significant. [Figure 4 and Figure 5].
In our study, the prevalence of TMD was more in female patients (51.9%) than in male patients (48.1%). Our study results were similar to that of other studies in which TMD was found to be 3-6 times more prevalent in women than in men (Biondi & Picardi, 1993; Mcneill, 1997). Our findings are consistent with a study by Bonjardim et al. that reported the percentage of women (57.43%) with TMD is higher than that of men (42.11%) (Bonjardim, Lopes-Filho, Amado, Albuquerque, & Goncalves, 2009). A study in Karnataka had concluded women (52.22%) were affected more with TMD symptoms compared to men (50.86%). The percentage of women (16.42%) with moderate TMD degrees was greater than men (10.34%) in the Karnataka population (Syeda, Katti, Syed, & Arora, 2012).
Garcia et al. in a sample of 122 students reported 68.85% of them were women with some degree of signs and symptoms (Garcia, Junior, & Pereira, 1997). Although a higher percentage of women than men had been diagnosed with TMD, the difference was not statistically significant. Concurrently, Syed et al. in a study of 250 outpatients found the difference was not statistically significant. Despite this, there have been some theories suggested for the female predominance in TMDs. According to the postulation, females are more subjected to mental and emotional disturbances than men. They are sensitive human beings and hence severe psychological symptoms were observed in women. Besides, females are more concerned about general health as they are suggested to seek treatment more often than men (Syeda et al., 2012).
In our study, higher prevalence of TMD was observed between age 31 and 40 years (36.7%) than other age groups. The least affected age group was in the range of 51-60 years (7.6%). Few investigations revealed the prevalence of TMDs varies with age. Children, adolescence and elderly demonstrated a low rate of TMD incidence, corroborating with the current study. In women, the severity of TMD symptoms was highly frequent after puberty and rose to the reproductive age group between 20-40 years (Bonjardim et al., 2009). Modi et al. reported 159 subjects of 21-22 years were the most affected with TMD as compared to other 97 subjects who were below 20 years (Modi, Shaikh, & Munde, 2012). A previous study among undiagnosed undergraduate students demonstrated a higher prevalence of TMD in students of 22-23 years (Hafila et al., 2017). The prevalence of TMD can affect any individual of any age group, with a higher proportion seen in women aged 20-45 years (Minghelli et al., 2014). The difference could be due to social background of the sample size population and methods of diagnosis.
In our study, similar to gender predilection, there was no statistically significant difference between age and TMDs. This concluded that age, as a factor, was not significant in the prevalence of TMJ disorder. Karthick et al. also found the same significant findings (Hafila et al., 2017). In contrast, Menghelli et al. and Bertoli et al. showed students in older age significantly were prevalent of developing TMDs (Bertoli et al., 2018; Minghelli et al., 2014). The different consensus obtained were more likely affected with the age limit of the subjects and severity of the TMDs.
Disc-condyle disorder (75.9%) is the most frequent sub-type of diagnosed temporomandibular disorders and the least recorded was degenerative disorders that were seen only in two patients in this study. 17 patients from the study had myofascial pain and dysfunction syndrome (21.5%). In study of Brazilian adolescence, 10.3% of the sample study was diagnosed with myofascial pain, which was more prevalent in girls. 8% had disc displacement and 3.5% had arthralgia. In contrary to this study, few studies had reported myofascial pain as the most common diagnosis for TMDs. No case of disc displacement and osteoarthrosis were detected (Bertoli et al., 2018; Franco-Micheloni, Fernandes, Gonçalves, & Camparis, 2015; Kobayashi, Gavião, Montes, Marquezin, & Castelo, 2014).
The limitations of this study include its small sample size distribution, geographic factors and associated signs and symptoms of TMDs were not mentioned. The present study is a pioneering study, therefore there is a need for long-term clinical investigations to be conducted in this region. This study will help to promote awareness of this disorder on the national level.
Conclusion
Within the limits of this study, TMDs were prevalent in females of age between 31 and 40 years, with disc-condyle disorder being the most prevalent type. TMD was significantly more common in women, but menarche was not associated with the prevalence of TMD in this sample. Considering that symptoms can be more prevalent with increasing age, clinicians and dental practitioners should be actively prepared to diagnose TMD signs at early stages for better therapeutic and clinical management.
Acknowledgements
We would like to thank saveetha dental college and hospital for the contributions and involvement through this study.
Authors contributions
Conceptualisation: Nor Masitah and Santhosh K; Methodology: Nor Masitah and Santhosh K; validation: Nor Masitah and Santhosh K; Analysis: Nor Masitah and Santhosh K; Draft preparation: Nor Masitah; Writing-review and Editing: Santhosh K; Visualisation: Arthi B
Conflict of interest
The authors declare that there was no conflict of interest for this study.
Funding Support
The authors declare that there is no funding support for this study.