Assessment of hospital anxiety and depression in newly diagnosed head and neck cancer patients in cancer institutes — A cross-sectional study
Abstract
Individuals often encounter psychological distress after a diagnosis of cancer, especially head and neck cancer (HNC). Worries regarding restricted functions, facial disfigurement, waiting time for investigation and duration of hospital stay for treatment make them feel awful. Often this feeling goes unnoticed and is underestimated. We aimed to assess the prevalence of the dreadful feeling in terms of anxiety and depression in newly diagnosed head and neck cancer patients. A cross-sectional study was conducted in two cancer-treating institutions in South India. About 357 freshly diagnosed HNC patients participated in the study. Pre-validated Hospital Anxiety and Depression Scale (HADS) was used to assess the anxiety and depression levels. Descriptive statistics was done to report socio-demographic, clinical variables and mean scores. Independent t-test and correlation test were done for comparison and association, respectively. Mean depression score for males and females was 11.481, 11.865, respectively. Mean anxiety score for males was 11.708 and 11.792 for females. There was a strong positive correlation between depression and anxiety score (0.864) among patients. There was no statistically significant difference in the mean anxiety and depression scores among gender, socioeconomic status, marital status and cancer stages (p>0.05). Newly diagnosed HNC patients had an abnormal level of anxiety and depression, which needs special attention and care during treatment for a better outcome.
Keywords
abnormal, borderline, distress, psychology, tobacco
Introduction
Head and neck cancer (HNC) among the ten most common cancers globally. About 57.5% of global head and neck cancers occur in Southeast Asia, mainly in India. In India, HNC accounts for 30% of all cancers (Kulkarni, 2013). Also, it accounts for one-fourth of male cancers and one-tenth of female cancers. Oral cancers are most common amongst all head and neck cancers due to increased use of tobacco, areca nut and alcohol etc. Poverty, illiteracy, advanced stages at presentation, lack of access to health care and poor treatment infrastructures in developing countries are responsible for the increased prevalence of HNC (Francis, 2018). Due to cancer pain, facial disfigurement, varying degrees of functional impairment related to speech, swallow, breath, taste and smell and financial burden for treatment; HNC patients less likely seek medical care. All these reasons account for higher rates of emotional distress during the illness, which could result in Suicide (Ahn, Park, & Lee, 2015; Robinson, Renshaw, Okello, Møller, & Davies, 2009). This emotional distress can be seen immediately after the diagnosis and also during the treatment course. Evidence has shown that the rate of depression among HNC patients is more than other cancer patients who ranged from 6% to 48% (Archer, Hutchison, & Korszun, 2008). Assessment of emotional distress at the and attention for the same at the diagnostic stage will help in better treatment outcome. Research on psychiatric morbidities at the diagnostic phase is limited in India. Hence, this study was taught to determine the level of psychiatric disorders in terms of anxiety and depression in newly diagnosed Head and Neck cancer patients.
Materials and Methods
The cross-sectional study was conducted in the department of oncology of Saveetha Dental College (a private institution) and Arignar Anna Cancer Institute, Kanchipuram (a government institution) from August 2019 to February 2020. The study commenced after obtaining ethical clearance from the institutional review board of Saveetha Dental College and Hospital, Chennai. A total of 357 adult patients with HNC were recruited for the study. Participants were selected using a convenient sampling method. Patients recently diagnosed (2-3 months) for head and neck cancer, present during the day and willing to participate included in the study. Patients under treatment or more than three months from diagnosis of HNC were excluded. Informed consent was obtained after explaining the purpose of the study by the principal investigator. The anonymity of the participants was maintained.
Socioeconomic status of the patients was obtained using a modified Kuppusamy scale 2019 (Saleem, 2019). For statistical purpose educational status was categorized as illiterate (not able to read, write and sign) and literate (able to read, write and sign). Similarly, the occupation was categorized as unemployed and employed (skilled, unskilled and self-employed). The family income was also categorized as < ₹4000, ₹4000-11,000 and > ₹11,000 (up to 80,000). A pre-validated and reliable Hospital Anxiety and Depression Scale (HADS) containing self-assessment questions were used (Karkal, Yadav, Kakunje, Mahatme, & Akhilesh, 2019).
The scale contains a question to assess anxiety and depression separately. Each question was measured using a Likert scale with scores ranging from 0-3. Anxiety and depression domain contained seven questions; where some are positive, and some are negative. The scale in English was translated into the vernacular language (Tamil). Retranslation was done by experts who know both the languages to check for the consistency of the content. An agreement kappa value of 0.83 was obtained among the experts. Interpretation of levels of anxiety and depression was made after summing up the scores. A score 0-7 represents normal; 8-10 represents borderline abnormal, and score 11-21 represents abnormal in each domain.
Statistical Analysis
Statistical analysis was done using Statistical Package for the Social Sciences version 23 (IBM Corporation., New York, USA). Descriptive statistics were used for reporting socio-demographic details, clinical variables and mean depression and anxiety scores. Pearson association and correlation were executed to find the relationship between depression and anxiety. An Independent t-test was done to compare the means of depression and anxiety across gender, socioeconomic status and cancer staging.
Results and Discussion
The mean age of the patients was 50± 15.57 years. About 69.7% of males and 30.25% of females participated in the study. Most of the patients were married (80.39%) and lived with their family at the time of assessment whereas 19.6% were single, widow or widower. About 64.7% of patients were employed, and 63.5% had <₹ 4000 family income. Most of them were uneducated (61.9%) and belonged to the lower middle class (Table 1).
|
Variables |
Categories |
Number of patients (%) |
|---|---|---|
|
Gender |
Male |
249 (69.74%) |
|
Female |
108(30.25%) |
|
|
Marital status |
Married |
287(80.39%) |
|
Single/widow/widower |
70(19.6%) |
|
|
Education |
Illiterate |
221(61.9%) |
|
Literate |
136(38.09%) |
|
|
Occupation |
Employed |
231(64.7%) |
|
Unemployed |
126(35.29%) |
|
|
Monthly family income |
<4000 |
227(63.5%) |
|
4000-11,000 |
102(28.57%) |
|
|
>11,000 |
28(7.8%) |
|
|
Socio-economic status |
Upper |
0 |
|
Upper Middle |
0 |
|
|
Lower Middle |
183(51.26%) |
|
|
Upper Lower |
77(21.56%) |
|
|
Lower |
97(27.17%) |
|
Variables |
Categories |
Number of patients (%) |
|---|---|---|
|
Habits |
With habits |
256(71.7%) |
|
Without habits |
101(28.29%) |
|
|
Weeks after diagnosis |
>4 weeks |
34(9.5%) |
|
4-8 weeks |
302(84.59%) |
|
|
8-12 weeks |
21(5.88%) |
|
|
Cancer staging |
Early (stage I and II) |
196(54.9%) |
|
Advanced (stage III and IV) |
161(45%) |
|
|
Treatment plan |
Surgery |
45(12.6%) |
|
Chemotherapy + Surgery |
243(68.06%) |
|
|
Surgery+Chemotherapy+Radiotherapy |
69(19.32%) |
|
Variables |
Categories |
Depression score |
Anxiety score |
||
|---|---|---|---|---|---|
|
Mean ± SD |
p-value |
Mean ± SD |
p-value |
||
|
Gender |
Male |
11.48 ± 3.97 |
0.818 |
11.70 ± 3.54 |
0.935 |
|
Female |
11.86 ± 3.60 |
0.824 |
11.79 ± 3.81 |
0.937 |
|
|
Socioeconomic status |
Lower middle |
11.02 ± 2.76 |
0.624 |
11.92 ± 3.78 |
0.534 |
|
Upper Lower |
10.34 ± 0.21 |
0.572 |
10.26 ± 0.17 |
0.345 |
|
|
Lower |
9.89 ± 0.40 |
0.452 |
10.01 ± 0.34 |
0.259 |
|
|
Marital status |
Married |
10.39 ± 0.34 |
0.166 |
9.29 ± 0.48 |
0.202 |
|
Single/widow/ widower |
11.02 ± 0.56 |
0.148 |
11.42 ± 0.21 |
0.193 |
|
|
Cancer staging |
Early |
10.84 ± 0.72 |
0.537 |
10.62 ± 0.43 |
0.279 |
|
Advanced |
11.33 ± 0.12 |
0.172 |
11.56 ± 0.26 |
0.421 |
|
|
Variables |
Chi-square value (χ2) |
p-value |
The correlation coefficient (r) |
p-value |
|---|---|---|---|---|
|
Depression score * Anxiety score |
371.65 |
0.000 |
0.864 |
0.000 |
About 71.7% of the patients had the habit of smoking/chewing/ alcohol. Most of them were interviewed at 4 weeks to 8 weeks (84.59%) from diagnosis. Most of the patients were in the early stages of cancer (54.9%). Chemotherapy and radiotherapy were the treatment plan for most of the study participants (68.06%). Almost all patients knew their diagnosis (Table 2).
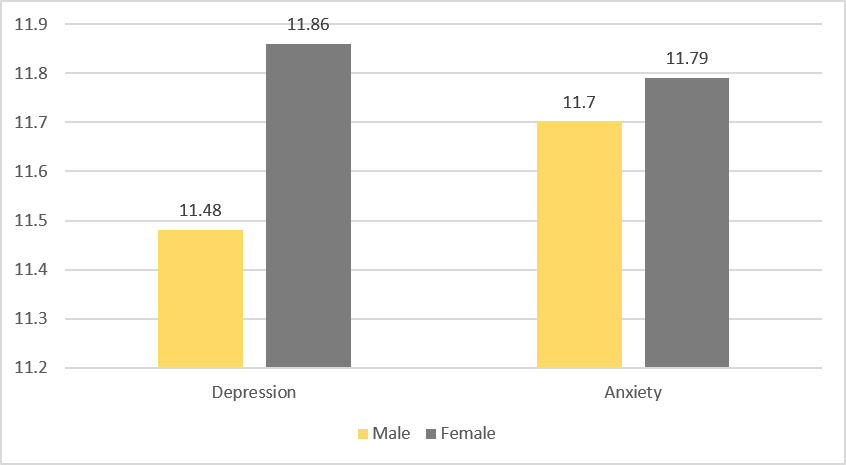
Mean depression scores of male and female was 11.481, 11.865, respectively. Mean anxiety scores for male was 11.708 and 11.792 for female (Figure 1). There was no statistically significant difference in the mean anxiety and depression scores among gender, socioeconomic status, marital status and cancer stages (p>0.05). However, mean scores were high in the lower middle class than the upper lower and lower class, patients living alone and with advanced stages of cancer (Table 3).
There are a statistically significant association and strong positive correlation (0.864) between anxiety and depression.
Individuals diagnosed with HNC have a higher level of anxiety and depression. This is one among the very few studies from South India, which has assessed the anxiety and depression level in newly diagnosed HNC using a standardized diagnostic tool.
The mean anxiety and depression scores are above score 11, which indicates an abnormal level of anxiety and depression among newly diagnosed HNC patients. Studies have reported higher prevalence rates of anxiety and depression at a pretreatment stage among HNC patients compared to patients undergoing treatment. However, these prevalence rates steadily declined over time (Lydiatt, Moran, & Burke, 2009; Wu et al., 2016).
The present study reported no difference in the anxiety and depression level among males and females (p>0.05). Evidence has shown no difference in gender bias in the prevalence of anxiety and depression. However, the prevalence was found higher in females compared to males. Lack of emotional support, lack of a social network, avoidant style of coping, advanced tumour stage and a lack of openness to discuss cancer in the family especially in married women are the reasons for these higher rates (Kugaya et al., 2000; Lydiatt et al., 2009).
In this study, young female patients had higher anxiety, but not depression scores. A similar finding was obtained by Noyes et al. (1990) using the Illness Distress Scale. They postulated that young adult patients might have more significant distress than older patients due to the effect of severe illness (i.e., cancer) on life plans. The above values are different from the ones reported by (Jones, Ford, & Jones, 2012) reported higher values in men for depression scores and these differences are also published in other studies in different languages and problems (Bocéréan & Dupret, 2014).
The HADS has been proved to be effective for its use in treatment response of anxiety and depression in clinically referred cancer patients. In one study, 86% of emotionally distressed patients were correctly identified by high anxiety or depression subscale score (Greer, Moorey, & Baruch, 1991). These findings suggest that the HADS is not only useful in screening for anxiety and depression in patients who have cancer but is also helpful in assessing changes in emotional distress and measuring the patient's response to treatment. When the higher cut-point score of more than 11 on the subscales is used, patients will warrant further psychiatric evaluation for anxiety and depressive disorders. This finding is similar to previous studies of major depression using other screening instruments (Bukberg, Penman, & Holland, 1984).
In this study, the HADS was the only screening instrument. Although it is useful in screening for anxiety and depressive symptoms, it cannot be used for diagnosis. This has been shown for other screening instruments that have been used in patients with cancer (Kathol, Mutgi, Williams, Clamon, & Noyes, 1990).
Studies have reported higher odds of anxiety and depression in patients living alone and with advanced stages of cancer with a cutoff point of 15 in HADS score (Ness, Hurley, & K, 2014; Zimmaro & Sephton, 2018). Our study showed no difference in the mean anxiety and depression scores among participants with different socioeconomic status, marital status and cancer staging. However, the mean scores were high for patients with advanced stages of cancer and patients who live alone. The high scores in advanced stages may be associated with a poor performance status (Kim, Roh, & Lee, 2016) malnutrition (Karvonen-Gutierrez et al., 2008) and physiological dysfunction (Rieke et al., 2017). High scores in patients living alone can be attributed due to the lack of social support and lack of emotional adaptation to cancer (Krebber et al., 2014).
This study showed a significant association between anxiety and depression and also showed a strong positive correlation (r=0.8), indicating that anxiety will always be associated with depression (Table 4). Also, translation of HADS to vernacular language produced no change in the relationship between anxiety and depression.
Our study had few limitations such as small sample size, cross-sectional design with the purposive sampling method. Further, a single-point assessment will not be sufficient to collect all the information throughout the course and treatment of illness.
Conclusion
This study showed a higher mean of anxiety and depression scores in newly diagnosed head and neck cancer patients. Considering these high scores, psycho-oncological and psychotherapeutic care will be needed as this present situation. Psychological care from the clinicians will help the patient for better treatment outcome, thereby increasing the survival rate.