Association between geographic location and periodontitis
Abstract
Periodontitis is one of the major reasons for tooth loss among adults globally, affecting their oral health-related quality of life. Ethnic and cultural variations play a major role in their oral hygiene practices which in turn reflects the oral health status.The present study aimed to find an association between geographic location and periodontitis. A retrospective cross-sectional study was conducted using patient records from September 2019 to April 2020. Consecutive digital case sheets with recorded periodontal index scores were used for data analysis. Descriptive statistics was done to present the results. Among 100 case records diagnosed with periodontitis, 64% were males, and 36% were females. Periodontitis was most prevalent in urban (58%) places. Among them established destructive periodontitis was most prevalent (46%). There found to be no statistically significant association between geographic location and periodontitis (p>0.05). This study concludes that periodontitis is more prevalent in urban males than rural males. It can be concluded that there is no role of geographic location on periodontal disease. However, there is a need for awareness of oral hygiene at this high time.
Keywords
Periodontitis, rural population, urban population, association
Introduction
Oral health is part of the overall health and has a significant impact on both the physical and psychological state. The efficacy of the use of oral self-care measures such as tooth brushing, flossing and use of interdental aids influences an individual’s oral hygiene maintenance. However, the improper use of these oral self-care methods would cause tooth abrasion and poor oral hygiene (Pratha & Prabakar, 2019).
Periodontal disease is a chronic inflammatory disease of the periodontium, and its advanced form is characterized by periodontal ligament loss and destruction of surrounding alveolar bone (Pablo, Chapple, & Dietrich, 2009). It is the main cause of tooth loss and is considered one of the two biggest threats to oral health (Benjamin, 2010). Periodontitis appears to be an infectious disease that has many characteristics of chronic disease, most forms progress slowly, and some aspects are not reversible, even if the infective agent is removed. There are approximately 800 species of bacteria identified in the oral cavity, and it is hypothesized that complex interaction of bacterial infection (Mohapatra, 2019) and host response, modified by behavioural factors such as smoking, can result in periodontal disease (Kumar & Preethi, 2017).
Gingivitis refers to the milder form of periodontal diseases. It is a reversible form of periodontal disease which is non-destructive. Destructive periodontal diseases include most commonly chronic periodontitis, followed by periodontitis associated with systemic diseases (Pavithra & Jayashri, 2019), aggressive periodontitis, and necrotizing periodontal diseases. Periodontitis serves as a risk factor for atherosclerosis, coronary heart disease, diabetes, respiratory infections and preterm low-birth-weight infants (Marya, 2010).
Lack of health education, awareness and infrastructure, poor oral hygiene practices, tobacco use, alcohol consumption, and insufficient oral healthcare facilities are the main culprits behind the poor oral health among the population of India (Gambhir, Sekhon, & Grewal, 2015). Hence, the prevalence rate of periodontal diseases in India is of great concern in public health dentistry. Dental plaque is the etiological factor for many chronic oral diseases, including periodontitis, as stated in many observational and experimental studies (Prabakar, John, & Srisakthi, 2016). People in rural areas neglect oral health as they lack awareness of dental diseases and also due to inadequate availability of dental services (Neralla et al., 2019).
Oral hygiene practices, especially in rural India, are still based on tradition and culture like the use of charcoal, mishri, miswak/chew sticks, and use of fingerssame (Samuel, Acharya, & Rao, 2020). Lack of awareness, use of tobacco and alcohol products, insufficient oral care contribute to poor oral health among rural populations (Mathew, Samuel, & Soni, 2020). In India, there are several challenges in delivering oral healthcare services to the rural population, including poor accessibility, lack of manpower, poverty and illiteracy. For instance, the dentist-to-population ratio in urban areas is 1:10,000,however, it is l: l,50,000 in rural areas which is slaved as inverse square law (Harini & Leelavathi, 2019). Moreover, there is a lack of enough data related to the rural population in India, which is necessary for planning oral health services. Therefore, it is necessary to assess oral health status and treatment needs in rural populations. Thus, the present study intended to find the association between geographic location and periodontitis.
Materials and Methods
Study design and setting
This University hospital-based retrospective study examined the records of patients during September 2019-April 2020 who had been diagnosed having periodontitis at Saveetha Dental College, Chennai. Ethical approval was obtained from the Institutional Ethics Committee. The consecutive case sheets of patients with Russell's periodontal index score were retrieved.
Data collection
Saveetha Dental College’s exclusive patient management software (DIAS, Dental Information Archiving Software) was used to identify 100 patients in the hospital database who were diagnosed with periodontitis. Relevant data such as patient age, sex and address was recorded. The geographic location (rural and urban) was categorized according to the National Census data. Data was verified by an external reviewer. The interpretation of Russell’s periodontal index (1967) includes 0 to 0.02 - clinically normal supportive tissues, 0.3 to 0.9 - simple gingivitis, 1 to 1.9 - beginning destructive periodontal disease, 2 to 4.9 - established periodontal disease, 5 to 8 - terminal disease.
Statistical analysis
Data were recorded in Microsoft Excel/2016 (Microsoft office 10) and later exported to the Statistical Package for Social Science for Windows (version 20.0, SPSS Inc., Chicago Ill., USA) and subjected to statistical analysis. Chi-square test was employed with a level of significance set at p<0.05.
Results and Discussion
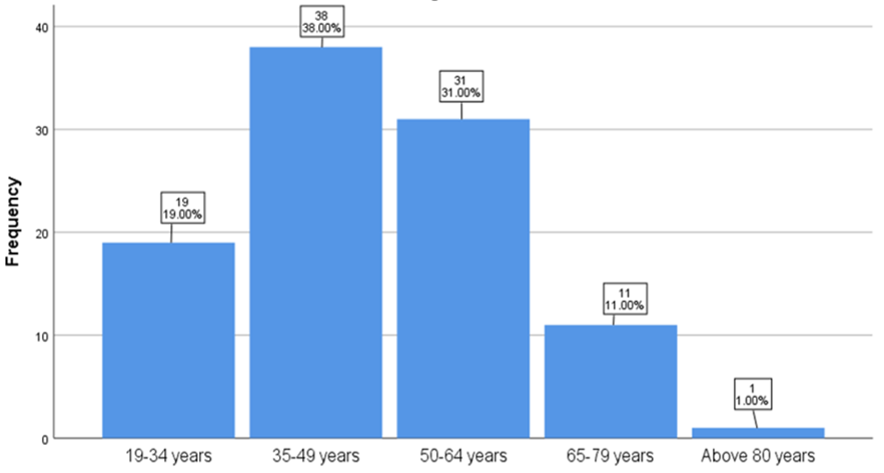
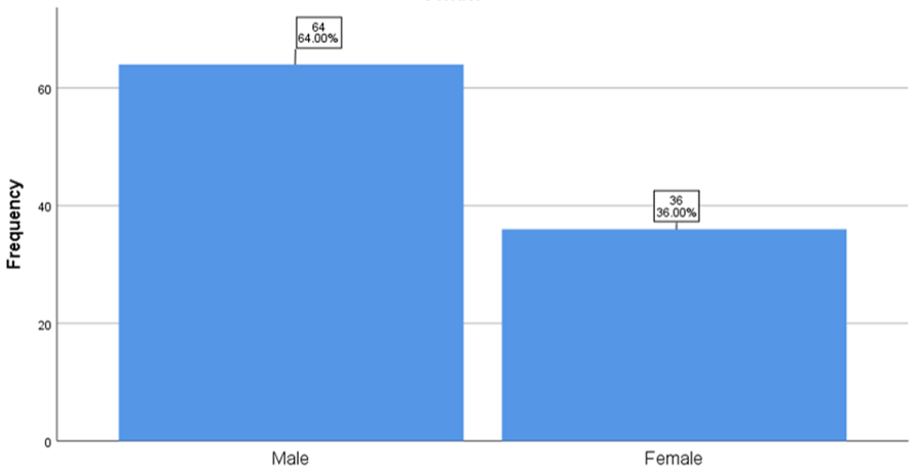
The final dataset consisted of 100 patients of Indian origin who were diagnosed with periodontitis. The mean age of patients who had periodontitis was 46.75 years (standard deviation = 13.494 years). The patient’s age ranged from 19 to 81 years. The patients were categorized into 5 age groups 19-34 years, 35-49 years, 50-64 years, 65-79 years, and above 80 years old for statistical analysis. Most of the patients (38%) belonged to 35-49 years Figure 1. There were more males (64%) compared to females (36%) Figure 2.
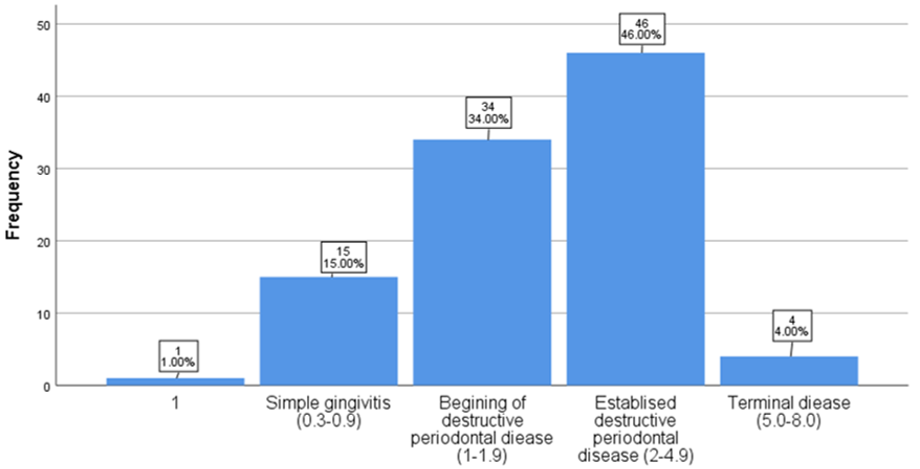
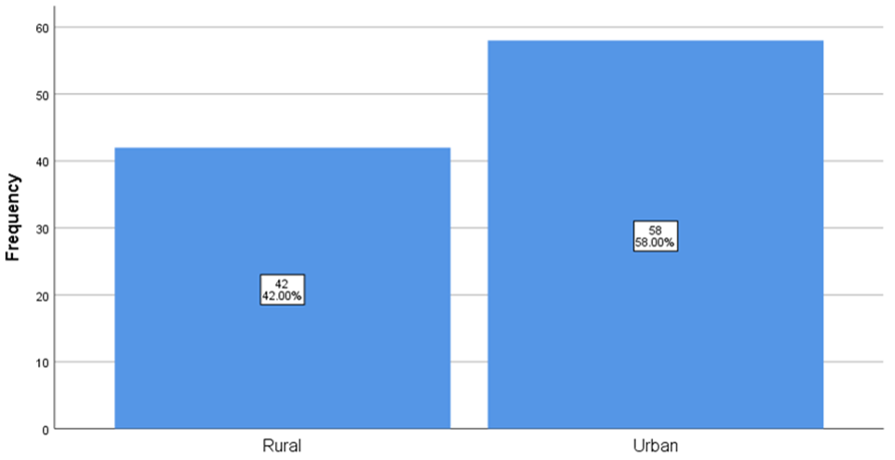
On analyzing the data records, there was a high prevalence of established destructive periodontitis (46%), followed by beginning destructive periodontal disease (35%), followed by simple gingivitis (15%) and terminal disease which had (4%) shown in Figure 3. Most of the patients visited the hospital were from urban areas (58%), and about 42% of patients were from rural areas (42%) shown inFigure 4.
Urban
A total of 58 patients were reviewed under Urban population out of which, the prevalence of simple gingivitis seen in urban population was 13.7%, beginning of destructive periodontal disease was seen in 36.2% patients. Established destructive periodontal disease was seen in 44.8%. Terminal diseases were the least and seen only in 3.4% of the total number of patients.
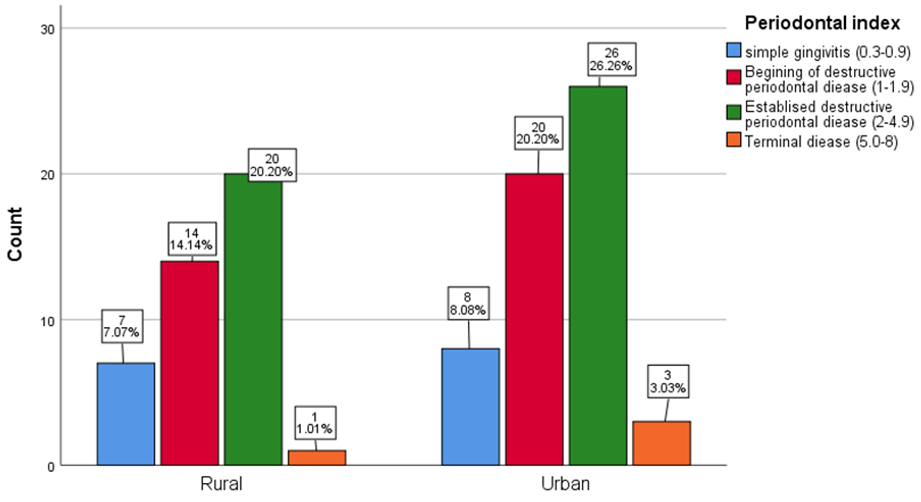
Rural
A total of 42 patients were reviewed under Rural population out of which, the prevalence of simple gingivitis seen in rural areas was 16.6%, The beginning of destructive periodontal disease was seen in 33.3% patients. Established destructive periodontal disease was seen in 47.6%. Terminal diseases were the least and seen only in 2.3% of the patients Figure 5. There was no statistically significant association elicited between geographic location and periodontists (p=0.865). The data for this retrospective study was based on patients seeking treatment at Saveetha Dental College. All the data was included without a sorting process; no bias was expected in the selection of patients. The current study aimed to shed light on the current scenario where the maintenance of oral hygiene is the main aims of oral health care, and the World Health Organization (WHO) in its report identified good oral health as an indicator of good health. They recommended various steps in order to improve oral health globally, and thus this can prevent periodontal disease (Petersen, 2003).
In this retrospective study, more males had periodontal disease than females. The findings are analogous to the study conducted by (Gambhir et al., 2015) and another study on the oral health status of Malaysian adults. The periodontal disease was most prevalent among men which can be attributed to their higher indulgence in adverse oral habits when compared to women.
Periodontal disease among females was (36.0%) this is an inconsistency to the study done by (Rao et al., 2016) had reported that periodontal health was shown to be compromised in females and could be attributed to poor nutrition, hormonal imbalance. However, a study done by (Bansal, Mittal, & Singh, 2015) reported that 59% males and 41% females which is in accordance to this study where the male had 64.0% and 36.0% were female having periodontal disease. The possible reason for this could be that males are less health-conscious and have smoking habits more than women.
In the current study, it was found that periodontal disease was higher in urban areas than in rural areas this is in accordance to the study done by (Antony, Akshaya, & Nair, 2020) where he found: Urban 173(42.3%), rural 118 (31.7%). The possible reason could be the negligence of self-oral care. As the results depend on several factors such as study designs, examiner calibration, microbial pathogens, disease activity, and multi factorial nature of periodontal diseases including age, gender, socioeconomic status, educational status, stress, and genetic factors, it is difficult to compare with observational studies.
Marya (2010) reported that the age group of 20-30 years high prevalence for periodontal disease (64.84%) whereas in the current study it was found to be the highest in of 35-49 years old (38.0%) which is contradicting and the possible reason could lack time for the oral care.
(Gambhir, Aggnur, Garg, & Veeresha, 2014) reported that the prevalence of early stages of PD involvement was 60.0%. The same author also quotes studies carried out in Trivandrum & Madras, which 90.3% and 95.0% respectively suffer from early stages of PD.
Considering that few studies analyzed the association between rural and urban areas and periodontitis in a prospective study, our retrospective study may be useful in clinical dentistry and used as baseline data for oral health education. Further prospective longitudinal studies with different ethnicity and cultural variations are needed to extrapolate the study results. The present study does not escape from limitations. Since it is a retrospective study, there might be some random errors.
Conclusion
Within the study limits, it was found that the prevalence of periodontal disease was high in urban male populations. Established destructive periodontal disease was more prevalent among them. There was no role of culture and ethnicity on periodontal disease. Personal oral habits in maintaining oral hygiene play a major role in periodontal disease. Thus, there is a need to create awareness among urban and rural males regarding the importance of oral hygiene for healthy periodontal tissue.
Acknowledgments
We take the immense pleasure to acknowledge Saveetha University for granting us permission to utilize the patient records for the study analysis.
Funding Support
The authors declare that they have no funding support for this study.
Conflict of Interest
The authors declare that they have no conflict of interest for this study.