Association of age and gender distribution in patients having class II caries resulting in root canal treatment in lower premolars and molars
Abstract
Caries or cavities is a breakdown of teeth due to acids made by bacteria. Individual tooth surfaces have different susceptibilities to caries which vary over time. Progress of caries towards the pulp leads to damage to the pulp. Caries 2 caries involve proximal surfaces of posterior teeth. The aim of the present study was to identify the association of age and gender distribution in patients having class II caries resulting in root canal treatment in lower premolars and molars. The data was collected from the DIAS - dental information archiving software. All case sheets were reviewed and findings are recorded. The data were tabulated using excel and analysed with the help of SPSS software. In this study, class II caries were common in the age group 60 to 70 years (73.9%). Males (63.8%) were more affected than females (36%). Lower molars (51%) showed a slightly higher incidence of class II caries when compared to premolars (49.4%). Within the limitations of the study, male patients showed a higher incidence of class II caries resulting in root canal treatment compared with female patients. 60 to 70 years was the commonly affected age group.
Keywords
class II caries, gender, lower premolar, lower molar, root canal treatment
Introduction
Class II dental caries is described as caries in the proximal (mesial or distal) surfaces of the premolars involving 2 or more surfaces that are mesio-occlusal, disto-occlusal, mesio-occluso- distal, mesio-occluso-distal buccal. Class II caries have a high incidence of pulp involvement which results in root canal treatment.
The noteworthy effect of caries on the population makes the disease a significant subject of comprehension. The improvement of caries is multifactorial, contingent upon many factors to advance its development. Specifically, the presence of microbes, a substrate for the microorganisms (food/sugar), the host's oral condition, the progress of time is the fundamental contributing elements in the development of caries (Ferraro & Vieira, 2010).
The effect of gastroesophageal reflux disease, bulimia cause the dissolution of the organic matrix of the tooth leading to softening of the tooth structure (Nasim & Nandakumar, 2018).
Recent studies showed that epidemiological and clinical investigations, using tools, for example, DMFT and DMFS scores, have uncovered a steady pattern in caries advancement, with females having higher predominance than males (Lukacs & Largaespada, 2006; Ramamoorthi, Nivedhitha, & Divyanand, 2015). Several components, like poor dietary and oral hygiene habits along with the social class, have been reported with caries occurrence (Adeniyi, 2009; Ramanathan & Solete, 2015).
Individual tooth surfaces have massively different susceptibilities to caries, with the pit and fissure (occlusal) surfaces the most common, and the smooth (labial and lingual) surfaces the least predominant (Chestnutt, Schäfer, Jacobson, & Stephen, 1998; Hannigan, 2000; Siddique, 2019). There is an extended risk of dental caries with age attributed by microbial and salivary conditions (Fure, 1998; Rajendran, 2019). It is believed that the prevalence of dental caries among adults is low compared with the pre and post-pubertal age groups (Hollander & Dunning, 1939; Nasim, 2018).
Most of the caries (recurrent) are related to the restoration than primary caries (Clarkson & Worthington, 1993; Kumar & Antony, 2018). In the previous study, it has been stated that there is evidence indicating various risk factors with gender bias, placing women at higher caries risk. (Martinez-Mier & Zandona, 2013; Ravinthar & Jayalakshmi, 2018). The ability of saliva to affect caries depends upon the quantity and composition of the secretion (Hicks, Garcia-Godoy, & Flaitz, 2004; Rajendran, 2019; Siddique, 2019).
This study spreads awareness, preventive measures with better management protocol and helps to Understand the association of age and gender with class II caries resulting in root canal treatment in lower premolars and molars. The aim of the present study was to identify the association of age and gender distribution in patients having class II caries resulting in root canal treatment in lower premolars and molars.
Materials and Methods
This retrospective study examined the records of patients from 01 June 2019 to 31st march 2020 who visited saveetha dental college and hospital. Ethical approval was taken from the institutional review board/SDC/SIHEC/2020/DIASDATA/0619-0320. The study sample included both male and female gender, predominantly south Indians.
We reviewed the patient's records and analysed data of 86,000 patients. The sample size was 71 patients, in the hospital database were diagnosed with class-II caries that progressed to Root canal treatment. Necessary data such as age, gender, class2 caries, caries in close proximity to the pulp were tabulated in the excel. Incomplete patient records were excluded.
Data were recorded in Microsoft Excel and exported to the statistical package of social science for windows (SPSS) and subjected to statistical analysis. Chi-square tests are used for comparison of groups.
Results and Discussion
All the required data was collected and analysed using SPSS software. About 44(63.8%) were Male and 25(36.2%) were female. Among the total 69 study population 1.45% belong to 20-30 years, 73.9% belong to 61-70 years and 24.6% belong to 71-80 years (Table 1)
|
Number of participants |
Percentage |
|
|---|---|---|
|
Gender |
||
|
Male |
44 |
63.8% |
|
Female |
25 |
36.2% |
|
Age |
||
|
20-30 years |
1 |
1.45% |
|
31-40 years |
0 |
0 |
|
41-50 years |
0 |
0 |
|
51-60 years |
0 |
0 |
|
61-70 years |
51 |
73.9% |
|
71-80 years |
17 |
24.6% |
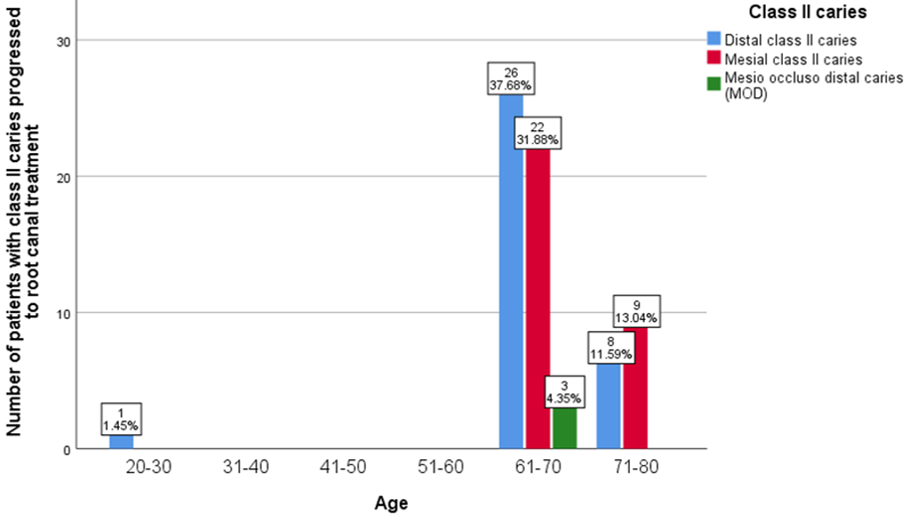
In this study, we observed class II caries treated with root canal treatment were in the age group between 60-70 years where distal class II is (37.68%) followed by mesial class II (31.88%) and mesio occluso distal caries (4.35%). In the age group between 71-80 years, distal class II caries is (11.59%) followed by mesial class II caries (13.4%). However, between the age group between 20-30 years, there is less incidence of class II caries that progressed to root canal treatment(1.45%). Correlation between age and class II caries resulting in RCT - chi-square (p) =.679 -p-value > 0.05 -statistically not significant. The X-axis represents the age, and Y-axis represents the incidence of class II caries and its progression to root canal treatment. Blue colour denotes distal class II caries, and red colour denotes mesial class II caries, green colour denotes mesio occluso distal caries. (Figure 1).
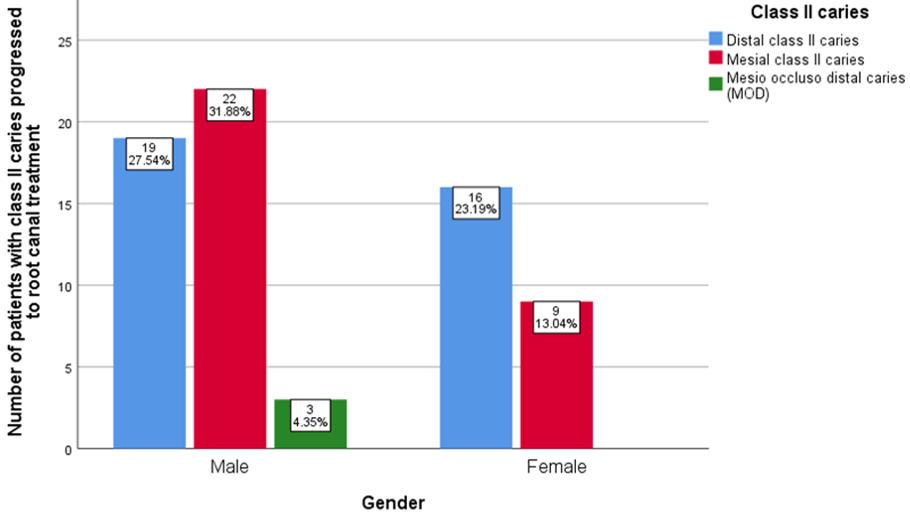
In association with gender, the analysed data revealed that class II caries progression to root canal treatment is observed to be higher in males compared to females. Males account for distal class II progression to root canal treatment is (27.54%) followed by mesial class -2 caries progression to root canal treatment is (31.88%) and mesio occluso distal caries [MOD] is 4.35%. Whereas in females distal class II caries progression to root canal treatment is (23.19%) and mesial class II caries progression to root canal treatment is (13.04%). Correlation between gender and class -2 caries resulting in root canal treatment - chi-square (p) = .152 -p-value > 0.005 - statistically not significant. The X-axis represents gender, and Y-axis represents an incidence of class II caries progression to root canal treatment. Blue colour denotes distal class II caries, and red colour denotes mesial class II caries, green colour denotes mesio occluso distal caries. (Figure 2).
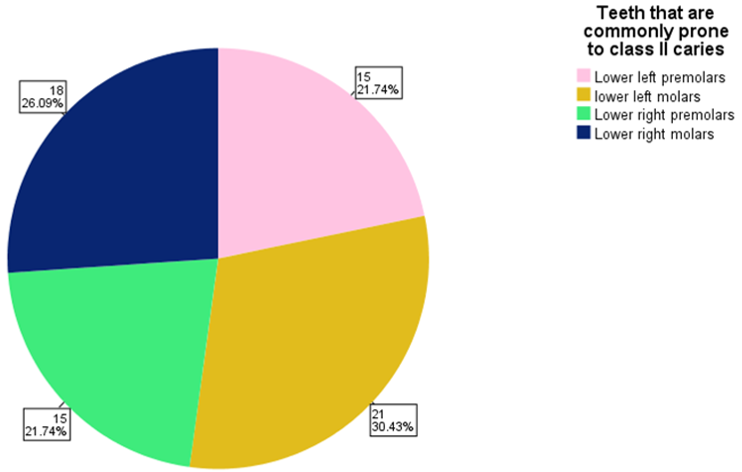
Among the teeth considered in this study lower left molars, 36,37 (30.43%) and lower right molar 46,47 (24.74%) are prone to class II caries when compared to lower left premolars 34,35(21.74%) followed by lower right premolars (21.74%) and least incidence of caries recorded in lower left third molar 38(1.45%). Light pink colour denotes lower left premolars, yellow colour denotes lower left molars, light green colour denotes lower right premolars, and dark blue colour denotes lower right molars. (Figure 3).
On data collection, it also revealed that most of caries involving the molar proximal surfaces have a poor prognosis, which leads to extractions and intentional root canal treatments. It is stated that neighbouring approximate tooth surfaces differed in caries susceptibility (Chestnutt, Schafer, Jacobson, & Stephen, 1996; Edward, 1997).
The results of earlier studies explained broadly about the incidence of all caries. However specific study on class-2 and its association is not well defined. In the previous study, it has been reported that caries has significant incidence among the age group for more than 65 years (80%) (Decerle, Nicolas, & Hennequin, 2013), and stated this could be due to factors like improper oral hygiene, nutrition and salivary hypofunction. The present study confirmed the same with respect to age. However, results are lower than what was obtained in a study conducted in 2009. Some studies showed age does not affect caries prevalence (Decerle et al., 2013).
Matrix metalloproteinases are produced by odontoblasts, and they also play a major role in the formation of dental caries and extensive periapical inflammation (Ramesh, Teja, & Priya, 2018). In case of trauma or due to any emergency, it is important for the dentist to consider the location and circumstances of the accident and suggest a proper transport medium for the avulsed tooth (Rajakeerthi & Nivedhitha, 2019).
Chlorhexidine is a broad-spectrum biocide. It is effective against gram-positive bacteria, gram-negative bacteria and fungi. The bactericidal effect is a result of the binding of this cationic molecule to negatively charged bacterial cell wall (Noor & Pradeep, 2016). Janani et al. showed consistent pulse oximeter readings in the study confirmed that pulp circulation and blood oxygen saturation can be detected by the pulse oximeter (Janani, Palanivelu, & Sandhya, 2020). It is recommended that endodontic therapy should be delayed on the traumatised teeth, and the affected pulp tissue should be considered vital unless apical radiolucency or sinus tract start to develop (Jose, P., & Subbaiyan, 2020).
At this time, the prevalence of caries in male was more compared to females according to this study. In the previous literature, it has been mentioned that women showed a higher incidence of caries (59.1%) than males (40.9%). This is justified as frequent hormonal fluctuation is experienced in women, type of diet, the difference in habits, rate of flow of saliva. This is in contrast to our study. Moreover, this study didn't do any targeted study on caries (Demirci, Tuncer, & Yuceokur, 2010).
Molars had the highest incidence of caries rate in all age groups due to deep pit and fissures, the large size of the crown (Ripa, Leske, & Varma, 1988). Maternal education, maternal age, location of residence and attitudes were positively associated with caries and oral hygiene index (Adeniyi, 2009). Caries distribution was higher in the maxillary jaw (62.4%) than in the Mandibular jaw (37.6%) in this study molars are more commonly affected ranging from (52.7%- 66.3%) which is due to deep occlusal fissures on the first and second molars showed the highest caries rate (Demirci et al., 2010). Compared to the present study results, distal class-2 caries are predominantly followed by mesial class-2 and MOD. It was reported that the distal surface of the posterior tooth commonly shows high incidence to caries (Stenlund, Mejare, & Kallestal, 2003).
Fast setting calcium hydroxide is used as pulp capping agents, and slow setting calcium hydroxide used as intra canal medicament should always be given after the completion of cleaning and shaping (Manohar & Sharma, 2018). A surgeon or a dental surgeon is always cautious in removing all the cystic remnants of the linings of the pathological lesion and remnants of caries or will be very careful in inspecting its margins after removing it because any remnants such as dental caries or periapical pathology that is left are going to cause further future progression and regrowth or recurrence of the lesion (Teja & Ramesh, 2019).
The limitations of the study are due to insufficient data with less sample size of 63, which can be expanded and diagnostic limitations. Data mostly relies on the case sheets available in the DIAS. The subject is not available for direct examination. In the future, the study can be performed in larger populations for a longer duration, better management protocol with the further scope of research. Thus, the study serves as evidence and add to the consensus that can be utilized for further studies at the larger population.
Conclusion
Mandibular molars are likely to experience caries compared to premolars, and Furthermore, Males have more class-2 caries teeth that resulted in root canal treatment than females. The most commonly affected age group is 60-70 years. On the other hand, molars are prone to distal caries.
Conflict of Interest
The authors declare that they have no conflict of interest for this study.
Funding Support
The authors declare that they have no funding support for this study.