Validation of Tamil Version of the Anemia Knowledge Questionnaire (AKQ)
Abstract
In India anemia is a common problem among Antenatal Women. In order to decrease maternal mortality, it is important to create knowledge among antenatal women. Varied instruments have been used to assess knowledge on anemia. However, there is a shortage for validated instruments in India for assessing anemia knowledge. The aim of present study is to develop a reliable and valid questionnaire to assess the knowledge of anemia to be used in antenatal women, reproductive women and adolescent girls. Before pretest researchers measured face validity and construct validity. The study was conducted in antenatal outpatient department of selected primary health centers at Thriuvallur district, Tamil Nadu, India. Subjects: Six nursing and one psychology expert, ten Village Health Nurse (VHN) and 100 antenatal mothers participated in the mission. During factorial analysis sampling adequacy was measured by using Kaiser- Meyer-Olkin (KMO) test (MSA) = 0.87 and Bartlett’s test of sphericity was X2 = 458.338 (p < 0.001). Varimax with Kaiser normalization rotation was performed and three factors were defined. The “general awareness” consists of four items (α = 0.79), anemia investigation and treatment component consists of six items (α = 0.81) and under diet and complication of anemia component, there is a five item factor (α = 0.89). In individual questions factor analysis, Cronbach’s alphas ranged from .84 and .86. 15.2% indicating total variance. There is no statistical significance between test and retest method. The questionnaire showed good validity and reliability (internal consistency and reproducibility), hence we can use this questionnaire among adults.
Keywords
Anemia, Knowledge, Scale, Validity, Reliability
Introduction
The continuous rise in anemia is presently a huge global health concern, especially in developing countries like India. Anemia causes serious health problems and it is the second most important cause of disability worldwide (World Health Organization, 2014). Nearly 50% of antenatal mothers has been affected by anemia in developing countries. In developing countries anemia is a major cause of morbidity and mortality among pregnant women and it leads to maternal and fetal complication (Khaskheli, Baloch, Baloch, Baloch, & Khaskheli, 2016; New & Wirth, 2015). Globally, more than 115,000 maternal and 591,000 prenatal deaths per year were due to anemia (Asrie, 2017). 54% of rural women and 46% of urban women were anemic in India according to National Family Health Survey - 2 (IIPS & ICF, 2018). Nearly half of the (57%) women has moderate level of anemia and 12 to 13% of them has mild, and severe anemia respectively in India (ICMR, 2004).
Maternal and fetal well-being are adversely affected during pregnancy as a result of anemia, and it leads to fetal death and morbidity. Breathing difficulties, fainting, tiredness, palpitations, and sleep difficulties were some symptoms frequently experienced by affected mothers (Canobbio et al., 2017; Lee, Zaffke, & Baratte-Beebe, 2001). Perinatal infection, pre-eclampsia, bleeding, post-partum cognitive impairment and behavioral difficulties incidence have also increased (Figueiredo et al., 2018; Wang et al., 2018). Particularly in the developing world, mortality risks have significantly increased because of the adverse perinatal outcomes including intrauterine growth retardation, prematurity, and low birth weight (Bangal, Aher, Bhosale, & Tuse, 2016; Sharma, Shastri, & Sharma, 2016). More negative impact on fetal growth is noticed due to anemia that developed during the third trimester than in the cases where anemia developed during the first and second trimester (Kumar & Asha, 2013; Tabrizi & Barjasteh, 2015).
Health promotion based proposal are emerging as a result of increase in chronic diseases like anemia in the last 25 years. Health promotion concept was thoroughly discussed and challenging scientific community to control chronic diseases. Adequate skills and knowledge is required to solve the problem of anemia and to improve their behavior on anemia control. Effective prevention and treatment will not be ensured by skills and knowledge. Understanding antenatal mother’s knowledge regarding anemia is supportive in clinical settings and research practice to evaluate teaching and to implement individualized education (World Health Organization, 2016).
Educational interventions meant to increase the knowledge of patients with chronic diseases can in turn will help to control, prevent and decrease the number of hospitalizations. Nevertheless, a recently published interventional study among pregnant women shows that Single educational interventional training for 45 minutes increased baseline knowledge regarding causes, signs and symptoms of anemia and dietary sources of iron from 21%, 23% and 40% to 64%, 66% and 72% respectively after the intervention (Nimbalkar, Patel, Thakor, & Patni, 2017). Self - care stimulus is emphasized to prevent anemia in antenatal women, reproductive women and adolescent girls. For this purpose, it is required to construct questionnaire that is simple and relevant to women, which will be aimed at verifying the knowledge they have regarding anemia.
In India, many studies have been executed to assess the knowledge related to anemia (Kumary et al., 2014; Priyankakumarai & Amoldeep, 2018). Knowledge barriers are the main reason for poor compliance of iron and folic acid (IFA) tablets uptake. Several studies (Kimiywe, Ahoya, & Kavle, 2017; Rai, Ratanasiri, & Arkaravichien, 2016) reported that during IFA tablets distribution, women did not receive adequate information. Qualitative study regarding anemia carried out in India (Chatterjee & Fernandes, 2014) showed that pregnant women were ignorant about the consequence of anemia on maternal outcomes. In most of the study, knowledge was assessed using not psychometrically validated questionnaire. For the Tamil population there are no valid and reliable instruments. Use of validated instrument can provide sound scientific conclusions from its results. To make sure that assessment questionnaire is valid and reliable appropriate psychometric methodology need to be followed. Taking into consideration these information, this study has been designed to develop reliable and valid questionnaire to assess the knowledge of anemia to be used in antenatal women, reproductive women and adolescents girls.
METHODS
Tool design
The questionnaire was developed in five stages: literature review, selection of variables, expert evaluation, pilot study, and evaluation of psychometric properties. Questionnaire was constructed based on the extensive review of literature on anemia knowledge, prevention and management (Angadi & Ranjitha, 2016; Sivapriya & Parida, 2015). The questionnaire was developed involving four health care professionals (An obstetrician, a nurse, and two nurse educators).
To assess the relevant application of the items, the language, the measurement scales used and to offer valuable suggestions for the inclusion of other items, the first version of questionnaire was sent to four experts in the areas of nursing and nursing education who have extensive experience in maternal and child health, medical surgical nursing and community health nursing. Pilot study was performed consequently with 30antenatal women. All antenatal women were from a selected primary health centre at Thiruvallur district who did not participate in the final study. The questionnaire was administered through self structured interview and self administered method, in order to establish the best method for performing the data collection. While administering questionnaire antenatal women were told to clarify their doubts and difficulty in understanding the questions with the researcher. The researcher noted down the questions which the subjects found difficult to understand and possible corrections were carried out.
The AKQ was developed for this study by the researcher to measure the antenatal women’s knowledge regarding general awareness about anemia (4 items), investigation and treatment (6 items), prevention and complication (5 items) of iron deficiency anemia. It consists of structured interview schedule and has 15 multiple choice questions. All questions were with four options of which one was the correct option. Score one was given for every right answer and score zero was given to every wrong answer. The distribution followed the pattern: General awareness about anemia score (4), Investigation and treatment score (6), and Prevention, control and complication score (5). Total possible score was 15.
Four experts rated the questionnaire in three point rating scale as not necessary (0), useful (1), essential (2). All comments were scored to calculate content validity ratio (CVR) and content validity index (CVI) using the following formula (Lawshe, 1975).
To calculate the CVR (a score for individual scale item)
Note:
ne = The number of experts who rated an item as essential.
N= the total number of experts.
The CVI is the mean CVR for all retained items.
CVI was calculated from the average score of the four experts, thus CVI of the AKQ was 0.978. The stability reliability of the tool was established by test-retest method at two weeks for 30 samples and the calculated correlation coefficient was 0.91. The equivalence reliability of the tool was established and the Cornbach’s alpha coefficient for this sample was 0.80.
The data collection period was February 2018 to June 2018. Approval to conduct the study was obtained from the Sri Ramachandra Medical College and Research Institute (Deemed University) institutional ethics committee for student project under REF:CSP/18/JAN/66/37. The study was conducted in antenatal outpatient department of Nemam and Sorancherry primary health centres at Thriuvallur district. Nemam and Sorancherry primary health centres are situated in the Poonamallee- Thiruvallur road at a distance of about 17 km away from Sri Ramachandra Medical College and Research Institute deemed to be university, Porur, Chennai, India.
Statistical Analysis
SPSS version 19.0 for Windows was used for the data examination. Means and standard deviations were used to explain the continuous variable. To find out the internal consistency of the tool Cronbach’s alpha coefficient (α) was used; values > 0.7 were considered as valid. To confirm reproducibility, test and re-test method was used and infraclass correlation coefficient (ICC) was performed with acceptable values close to 1. Reliability values > 0.2 (25) were considered as acceptable while calculating the item-total correlation test. To validate the tool, following test were computed. To find out the number of factors to be extracted, Load factor analysis was completed, load values ≥0.3 were used as standard parameters. To determine sphericity index, Bartlett’s test was rundown with a significance level p < 0.05. Adequacy of sampling was measured with the help of the measures of sampling adequacy (MSA) of Kaiser-Meyer-Olkin (KMO), ≥0.60 MSA values were considered as satisfactory. Lastly, number of factors was extracted by scree plot analysis.
Results
A total of 100 antenatal women’s were conveniently selected for the study. Average age of the participants was 25.6 years, the minimum age of the participants was 18 years and maximum age of the participants was 35 years. 45.0% of antenatal women was in the age group of 21-25 years and 30.0% of them were in the age group of 26-30 years. Majority (70%) of them were educated up to higher secondary education. Most of the antenatal women 86 (86.0%) were housewives. 28% of them had Hemoglobin levels less than 10 g/dl> Almost 52% of them had Hemoglobin levels 10-12 g/dl, while only 5% of them had Hemoglobin levels above 12 g/dl. Each participant was interviewed separately and privately while being made to sit comfortably in chair. The interview lasted for 30 to 40 minutes. Strict confidentiality was maintained throughout the interview, the language used for the interview was Tamil. Distribution of antenatal women according to their demographic and maternal variables is shown in Table 1 Factor Analysis.
|
Maternal variables |
% |
|---|---|
|
Age in years |
|
|
18-20 21-25 26-30 31-35 |
11.0 45.0 30.0 14.0 |
|
Type of Family |
|
|
Nuclear family Joint family |
35.0 65.0 |
|
Hemoglobin level after completion of 32 weeks of gestation |
|
|
Not done < 8g/dl 8.1-9.9 g/dl 10-12 g/dl 12.1-15 g/dl |
15.0 6.0 22.0 52.0 5.0 |
|
Number of pregnancy |
|
|
One Two Three More than three |
44.0 39.0 9.0 8.0 |
|
Gestational age in trimester |
|
|
First trimester Second trimester Third trimester |
15.0 34.0 51.0 |
|
During present pregnancy have a history of |
|
|
N/A Pregnancy induced hypertension Gestational diabetes Ante partum hemorrhage Twin pregnancy Hyper emesis gravidarm |
79.0 2.0 4.0 1.0 1.0 14.0 |
|
Sub-dimensions Item number |
Item |
Factor loading |
Variation explained (%) |
|---|---|---|---|
|
General awareness about anaemia |
1.What is anemia in pregnancy? |
.829 |
35.530 |
|
2.What is the most common cause of anemia? |
.719 |
||
|
3.Which of the following affects the pregnant women at a higher risk of acquiring anemia? |
.563 |
||
|
4.Which of these are signs of anemia? |
.736 |
||
|
5.What is the normal hemoglobin level during pregnancy? |
.792 |
||
|
Treatment |
6.How long should the patient take treatment for the cure of anemia? |
.894 |
8.841 |
|
7.What is the first line treatment of anemia? |
.804 |
||
|
8.What will be the treatment for severe anemia? |
.673 |
||
|
Diet and complication |
9.What type of diet is ideal for anemia? |
.700 |
7.286 |
|
10.Which of the following is rich in iron? |
.800 |
||
|
11.Which of the following is rich in Vitamin C? |
.853 |
||
|
12.Which element hinders the iron absorption? |
.821 |
||
|
13.Which element enhances the iron absorption? |
.670 |
||
|
14.What is the maternal complication of severe anemia during pregnancy? |
.795 |
||
|
15.What is the fetal complication of severe anemia in a mother? |
.875 |
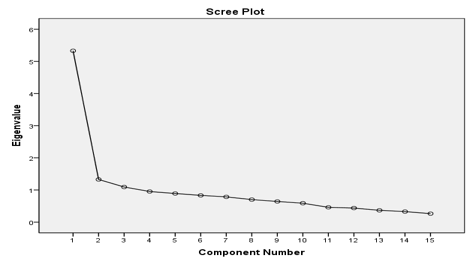
Factor analysis, particularly principal component analysis was performed to assess construct validity in order to establish the credentials deliberated by the questionnaire and observe the significance of the total scores. Kaiser-Meyer-Olkin measure of sampling adequacy was .873 and Bartlett’s test of sphericity, approx. Chi-Square was 458.338 with p < 0.001. Factor loading of <0.40 (total: 5 items) in the factor analysis were excluded from individual item and sub-scale items. Three factors were extracted from varimax rotation. The AKQ 15 questions appear to determine 3 primary factors since only these 3 primary factors have an Eigenvalue of at least 1(Scree plot) as shown in Figure 1. The distribution followed as six items in first factor, 5 items in the second factor and 4 items in the third factor. Total variance accounted for each factor was 35.5%. All the items had unrotated factor loading more than .4. The total variance of three factors was 52%. The final questionnaire consisted of three dimensions considering the factor analysis, one as general aspect, second dimension as identification and treatment and third dimension including prevention and complication aspects. The Table 2 shows the results of the factor analysis for AKQ.
The reliability of the scale and each sub-dimension was calculated using the Cronbach alpha coefficient. During the analysis the Items that had an item-total correlation of <0.40 were reframed and included in the measure. For every item, a Cronbach coefficient alpha value of >0.69 and <0.95 was defined as acceptable. Ultimately, no items were excluded from the scale.
The internal consistency of the complete scale Cronbach alpha values was 0.93, the sub scale General awareness about anemia scale value was0.79, Treatment value was 0.81 and Diet and complication value was 0.89. According to (George & Mallery, 2003) rules reliability of the complete scale was excellent, while the sub scale reliability were good and acceptable.
Discussion
To the best of our acquaintance, this is the first study in India with regard to development and validation of an anemia knowledge questionnaire. This study helped to develop reliable and valid questionnaire consisting of 15 items for assessment of knowledge on anemia among women of reproductive age (WRA). The early and ultimate appraisal of the questionnaire showed excellent content validity and test-retest reliability among the Tamil speaking population.
Globally 41.8% of pregnant women was affected by anemia. Among the 16MM (16 major pharmaceutical markets) India has the highest prevalence of anemia. The prevalence is even higher among Indian women, with around 50% of women having low hemoglobin levels. The major apprehension about the undesirable effects of anemia on pregnant women is the faith that this group is at higher risk of perinatal mortality and morbidity (Benoist, 2008; Globaldata, 2017).
According to National Family Health Survey 3 only 23% of pregnant women has consumed Iron and folic acid tablets during their pregnancy for at least 90 days though the Iron and folic acid treatment to pregnant women was good. Insufficient awareness concerning anemia and iron rich food, avoidance of iron supplements due to misconceptions, pessimistic attitudes towards antenatal visits, importance of a healthy diet, and iron and folic acid intake during pregnancy are the main causes for the negative impact and low compliance among pregnant women. Hence the present study was carried out to construct a questionnaire that perfectly reflects culturally reliable social norms values and viewpoints in an attempt to determine individual knowledge levels.
Anemia knowledge questionnaire was developed with 15 items for the assessment of the antenatal women’s level of knowledge and it was standardized to use among antenatal women with anemia and without anemia, adolescents and woman of reproductive age. Standardization was done both in English and local Tamil language. AKQ can be utilized as a screening tool to assess the knowledge and to plan, implement and evaluate the educational interventions to improve the knowledge of the reproductive age women before pregnancy, during pregnancy and after pregnancy thereby enabling them to be active participants in the maintenance of healthy reproductive period. Antenatal women’s knowledge regarding general awareness about anemia, investigation and treatment, prevention and complication of iron deficiency anemia, these three domains of the questionnaire analysis in detail thereby the comprehensive knowledge essential to empower women’s passionate involvement in disease management can be evaluated by the questionnaire.
Conclusion
The prevalence of anemia is still peaking in developing countries like India. Studies in such environments show us that the relation between health seeking behavior and knowledge is not adequately addressed. The questionnaire newly developed and validated through this study serves twin purposes namely assessing knowledge regarding anemia and educating the vulnerable in a way developing health seeking behavior as part of the anemia prevention and control program.
Acknowledgement
None.
Funding Support
The authors declare that they have no funding support for this study.
Conflict of Interest
The authors declare that there is no conflict of interest for this study.